The Diagnostic Paradigm in Psychextrics: From Clinical Observation to Biological, Behavioural, and Emotional Mapping
The End of Psychological Observation as Diagnosis
BY: OMOLAJA MAKINEE
For much of modern psychological history, diagnosis has relied upon a remarkably simple premise.
- Observe behaviour.
- Listen to self-reported experiences.
- Identify patterns.
- Assign a category.
- The patient speaks.
- The clinician interprets.
- The diagnosis emerges.
This methodology has shaped Psychiatry, Personality Psychology, Behavioural Science, and countless therapeutic frameworks for generations.
Yet beneath its apparent sophistication lies a profound limitation. Observation only reveals output. It does not reveal origin. Human beings can display identical behaviours while being driven by entirely different biological mechanisms.
Likewise, individuals with vastly different outward presentations may be governed by the same underlying behavioural architecture.
Psychextrics identifies this as the central failure of traditional clinical observation.
The problem is not that observation lacks value. The problem is that observation alone cannot reveal causation. It can only reveal appearance.
What clinicians often interpret as motive, personality, intention, disorder, compatibility, or pathology may simply be the visible surface of deeper memory systems operating beneath conscious awareness.
Under Psychextrics, diagnosis therefore shifts away from observation and toward architecture.
The question is no longer: “What behaviour was observed?“
The question becomes: “Which memory system originated the behaviour?“
1. Memory as Active Behavioural Architecture
The foundation of this diagnostic shift begins with a redefinition of memory itself. Within Psychextrics, memory is not historical residue. Memory is not an archived-trace recording. Memory is not stored experience waiting for retrieval. Memory is active behavioural architecture.
Every memory system continuously participates in the construction of present reality.
- Biological-memory shapes physiological state.
- Behavioural-memory shapes interpretations and prediction.
- Emotional-memory shapes saliency and urgency.
The organism never experiences reality from a neutral position. Reality is constantly filtered through inherited structures, adaptive modifications, behavioural reconstructions, and emotional weighting systems.
What appears to be a simple decision is often the final expression of multiple memory systems interacting simultaneously. The consequence is profound.
Human behaviour cannot be understood through observation alone because observation only captures the final display. It does not capture the architecture that produced the display.
2. The Deconstruction of Clinical Observation
Traditional psychological method in Behavioural science largely operates through descriptive categorisation.
- A patient reports symptoms.
- The clinician observes behaviour.
- Patterns are grouped.
- Labels are assigned.
- The diagnosis emerges from interpretation.
Psychextrics argues that this methodology inevitably creates diagnostic blindness. Two individuals may exhibit identical outward behaviours.
- Both may avoid social gatherings.
- Both may struggle with intimacy.
- Both may appear emotionally detached.
Yet their underlying biological architectures may be entirely different.
- One individual may possess behavioural-memory configurations centred around sensory overload.
- Another may possess emotional-memory configurations centred around threat saliency.
- A third may possess biological-memory disturbances rooted in endocrine dysfunction.
The visible behaviour appears identical. The origin is completely different.
Observation alone cannot distinguish between them. The diagnosis therefore risks categorising symptoms rather than identifying causes. Psychextrics seeks to reverse this process.
Rather than diagnosing outward behaviour, it diagnoses the memory systems generating the behaviour under psychextrical method.
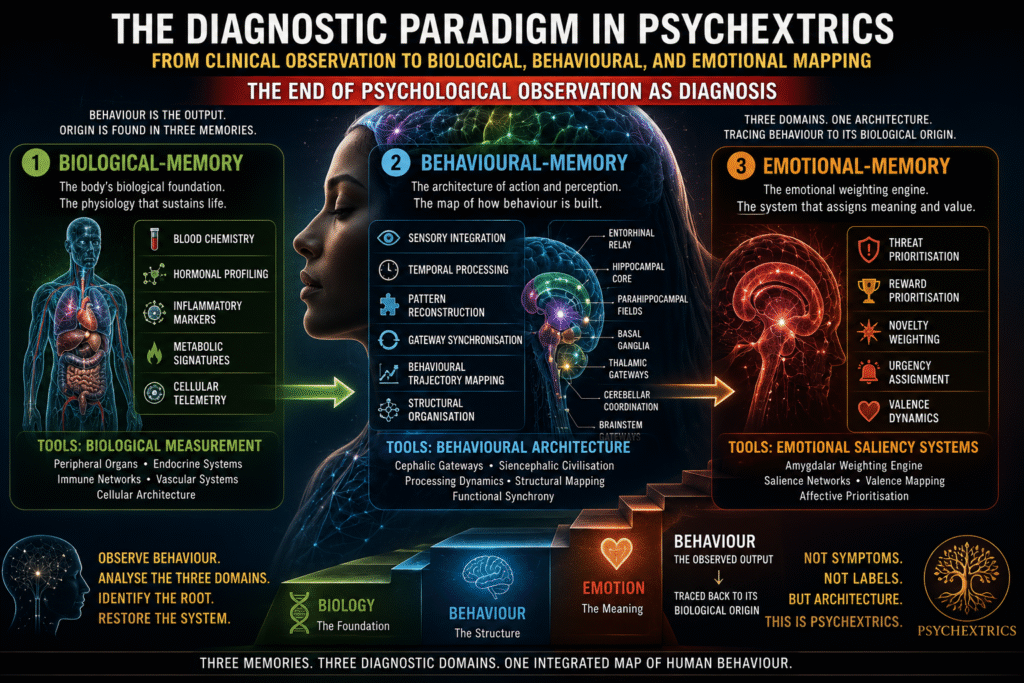
3. The Three Diagnostic Domains
The Psychextric diagnostic model is built upon the tripartite architecture of memory.
- Biological-Memory.
- Behavioural-Memory.
- Emotional-Memory.
Each layer possesses its own anatomy.
- Its own operating rules.
- Its own pathology.
- Its own diagnostic methodology.
The first domain is Biological-Memory.
This includes the peripheral organs, endocrine systems, immune networks, vascular systems, and cellular architecture of the body.
Its primary diagnostic tools involve biological measurement.
- Blood chemistry.
- Hormonal profiling.
- Inflammatory markers.
- Metabolic signatures.
- Cellular telemetry.
The second domain is Behavioural-Memory.
This includes the cephalic gateways and the Siencephalic civilisation. Its diagnostic tools involve behavioural architecture itself.
- Sensory integration.
- Temporal processing.
- Pattern reconstruction.
- Gateway synchronisation.
- Behavioural trajectory mapping.
- Structural organisation.
The third domain is Emotional-Memory.
This domain belongs primarily to the Amygdalar weighting engine. Its diagnostic focus involves emotional saliency systems.
- Threat prioritisation.
- Reward prioritisation.
- Novelty weighting.
- Urgency assignment.
- Valence dynamics.
Together these three domains create a comprehensive diagnostic staircase capable of tracing behaviour back to its biological origin.
4. From Descriptive Psychiatry to Spectral Pathology
One of the most radical implications of Psychextrics is its proposed transformation of Psychiatry. Traditional psychiatric systems largely classify behavioural outputs.
- They describe symptom clusters.
- They group common presentations.
- They identify recurring behavioural patterns.
Psychextrics proposes a different direction.
Rather than describing behavioural outcomes, Psychiatry becomes the science of behavioural-memory architecture.
The focus shifts toward cephalic gateway organisation.
- Subcortical integration.
- Spectral variation.
- Pattern reconstruction.
- Behavioural synchronisation.
Under such a framework, disorders become architectural phenomena rather than descriptive labels.
The clinician no longer asks: “What symptoms are present?“
Instead, the clinician asks: “Which cephalic gateway architecture produced these symptoms?“
This transition transforms Psychiatry from symptom classification into structural pathology.
5. The End of Personality Speculation
An equally profound transformation occurs within personality science.
For centuries, personality has been interpreted largely through observation.
- Traits.
- Temperaments.
- Styles.
- Profiles.
- Narratives.
- Questionnaires.
- Self-reports.
Psychextrics argues that personality is often confused with its emotional expression.
- People describe themselves.
- Others describe them.
- Observers assign categories.
Yet these observations reveal only the visible output of emotional-memory. They do not necessarily reveal the underlying emotional architecture itself.
The Psychextric model therefore proposes direct mapping of emotional-memory through HIM-HFI dynamics. Instead of inferring emotional tendencies from behaviour, emotional systems become measurable through their biological expression.
The goal is not merely to interpret personality. The goal is to identify the molecular mechanics that regulate emotional saliency.
In this framework, emotional-memory replaces personality speculation with emotional architecture.
6. The Relational Arena and the Illusion of Compatibility
Nowhere is diagnostic blindness more visible than within modern relationship environments. Particularly within digital dating systems.
Contemporary dating platforms create the appearance of compatibility through shared narratives.
- Individuals construct profiles.
- They select preferences.
- They write descriptions.
- They present intentions.
Yet beneath these narratives often exist radically different motivational architectures.
Several individuals may present identical social scripts while pursuing entirely different outcomes.
- One seeks physical novelty.
- Another seeks lifelong partnership.
- Another seeks economic stability.
- Another seeks companionship.
- Another seeks emotional safety.
- Another seeks social belonging.
The language used may appear identical. The motivations may be completely different. The result is what Psychextrics identifies as narrative convergence.
Different motivational systems adopting the same social language.
Compatibility becomes increasingly difficult to determine because observers evaluate scripts rather than architecture.
7. Why Motives Cannot Be Reliably Inferred
Human beings possess extraordinary abilities to modify presentation.
They can rehearse.
- Adapt.
- Mask.
- Perform.
- Conceal.
- Mimic.
- Strategically communicate.
Yet the underlying memory systems remain active regardless of narrative performance.
An individual may describe themselves as seeking casual intimacy. Another may describe themselves using identical language. Their biological trajectories may still be entirely different.
- One may be driven by novelty saliency.
- Another by emotional safety.
- Another by resource acquisition.
- Another by loneliness reduction.
The observable narrative remains constant. The biological architecture differs.
This distinction forms one of the central principles of Psychextric diagnostics. Narratives can be modified. Architectures cannot be disguised as easily.
8. Mapping the Architecture Beneath the Script
The Psychextric solution is to bypass narrative interpretation entirely. Instead of asking what an individual claims to want, the focus shifts toward how their memory systems behave across changing environments.
- How do emotional weighting systems respond?
- How do behavioural gateways reorganise?
- How do biological systems fluctuate?
- How stable are behavioural trajectories?
- How do saliency networks react to environmental change?
By tracing the interaction between Biological-Memory, Behavioural-Memory, and Emotional-Memory, the underlying motivational architecture becomes visible.
The narrative becomes secondary. The architecture becomes primary.
This represents a fundamental inversion of traditional psychological methodology.
9. The Diagnostic Separation of Appearance and Origin
The most important contribution of the Psychextric diagnostic paradigm is its insistence on separating appearance from origin.
- Behaviour is appearance. Memory architecture is origin.
- Symptoms are appearance. Gateway organisation is origin.
- Emotional display is appearance. Valence mechanics are origin.
- Narrative is appearance. Biology is origin.
Traditional observation often begins and ends with appearance. Psychextrics begins with appearance and works backward toward architecture.
Only by identifying the originating memory system can diagnosis move beyond description and approach explanation.
Conclusion: The Future of Diagnosis
The diagnostic paradigm proposed by Psychextrics represents a transition from observation-based interpretation to architecture-based analysis.
- Biological-Memory reveals the physiological history of the organism.
- Behavioural-Memory reveals the structural organisation of perception, prediction, and action.
- Emotional-Memory reveals the weighting systems that determine saliency, urgency, attraction, and threat.
Together these three domains form a comprehensive diagnostic framework.
The clinician no longer relies exclusively upon what a patient says. Nor solely upon what a patient does. Instead, diagnosis becomes the study of the biological, behavioural, and emotional architectures generating both speech and action.
In this framework, observation remains useful but loses its privileged status. Behaviour becomes evidence. Not explanation. Narratives become clues. Not truth. The true object of diagnosis becomes the living architecture of memory itself.
Because human beings may imitate each other’s language, mimic each other’s behaviour, and reproduce identical social scripts, yet the underlying memory systems that generate those performances remain uniquely their own.
The future of Psychextrics therefore lies not merely in interpreting behaviour, but in tracing behaviour back to the biological, behavioural, and emotional engines from which it emerges.
- The body records.
- The gateways organise.
- The amygdala prioritises.
- The hippocampus reconstructs.
- The thalamus narrates.
And within that hierarchy lies the foundation of a new diagnostic science.
Back to: 👇