The Tripartite Stratification of Memory and Disease: Biological-Memory, Behavioural-Memory, and Emotional-Memory
Why Memory Cannot Be Reduced to a Single System
BY: OMOLAJA MAKINEE
One of the most persistent problems in the study of behaviour is the tendency to treat memory as a singular phenomenon.
- A memory is remembered.
- A memory is forgotten.
- A memory is stored.
- A memory is recalled.
Such language creates the impression that all memories belong to the same category and originate from the same biological machinery. Psychextrics rejects this assumption.
Memory is not singular. Memory is stratified. Different forms of memory emerge from different anatomical territories.
- They obey different biological rules.
- They possess different diagnostic signatures.
- They produce different pathological outcomes.
Most importantly, they participate in behaviour through fundamentally different mechanisms.
To understand disease, behaviour, and consciousness, memory must first be separated into its primary biological layers.
Within Psychextrics, three distinct strata govern the architecture of memory:
- Biological-Memory.
- Behavioural-Memory.
- Emotional-Memory.
These three domains form a hierarchical system extending from the peripheral organs to the cephalic gateways and finally to the amygdalar weighting engine.
Together they govern the entire landscape of behavioural existence.
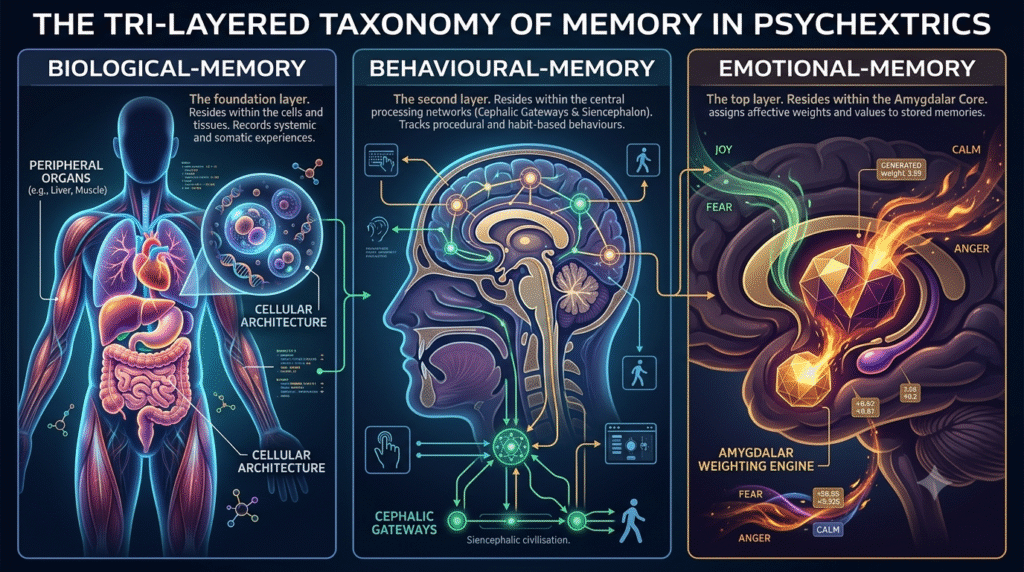
1. The Tri-Layered Taxonomy of Memory
- The first layer consists of Biological-Memory. This layer resides within the peripheral organs and the cellular architecture of the body.
- The second layer consists of Behavioural-Memory. This layer resides within the cephalic gateways and the Siencephalic civilisation.
- The third layer consists of Emotional-Memory. This layer resides within the Amygdalar Core.
These layers are connected. They influence one another. Yet they remain structurally distinct.
- Each possesses its own anatomical territory.
- Each possesses its own inherited framework.
- Each possesses its own adaptive mechanisms.
- Each possesses its own disease processes.
The resulting hierarchy may be viewed as a biological staircase.
- Biological-Memory forms the foundation.
- Behavioural-Memory emerges from the foundation to regulates the expression of Biological-Memory.
- Emotional-Memory emerges from the foundation to regulates the expression of both.
The organism therefore does not behave through memory alone. It behaves through the interaction of three separate memory systems operating simultaneously.
2. Biological-Memory: The Foundation of Living History
The deepest layer of memory exists within the organs of the body.
- The heart.
- The liver.
- The lungs.
- The kidneys.
- The gastrointestinal tract.
- The endocrine system.
These structures continuously accumulate biological history.
- Every meal.
- Every toxin.
- Every infection.
- Every injury.
- Every adaptation.
- Every hormonal fluctuation.
- Every metabolic challenge.
All leave enduring biological traces. Within Psychextrics, these traces constitute Biological-Memory.
Biological-Memory is built through the interaction between inherited organisational frameworks and adaptive molecular modifications.
- The inherited framework emerges through GIM-HIM architecture.
- The adaptive content emerges through EIM-HFI modulation.
Together they create the living biological history of the organism.
This history is not symbolic.
- It is cellular.
- It is molecular.
- It is physiological.
The body remembers through what it becomes. Not through what it stores.
- A liver remembers chronic alcohol exposure because its molecular architecture has been altered.
- A cardiovascular system remembers prolonged stress because vascular and endocrine adaptations have accumulated.
- A gastrointestinal system remembers dietary history through ongoing microbial and cellular modification.
The memory is the structure itself.
3. Why Biological Disease Can Be Diagnosed Through Blood
The unique position of Biological-Memory explains one of the most powerful tools in medicine.
The blood test.
Blood circulates through virtually every organ system. As it moves, it carries molecular fragments of biological history.
- Inflammatory markers.
- Hormonal profiles.
- Metabolic by-products.
- Enzymatic signatures.
- Cellular degradation products.
- Immune activity.
These circulating signals provide direct access to Biological-Memory.
When clinicians evaluate liver enzymes, kidney function markers, inflammatory proteins, or endocrine outputs, they are effectively reading the operational history of the body’s biological systems.
The bloodstream functions as a continuous telemetry network. It transports information from the source itself. This is why a single blood draw can reveal enormous amounts of information about systemic health.
The biological source and the diagnostic medium remain directly connected.
4. Behavioural-Memory: The Architecture of Behaviour
The second layer emerges when biological information migrates into the cephalic hierarchy. At this stage, memory ceases to be purely physiological. It becomes behavioural.
Behavioural-Memory resides within the gateways of the five cephalic architecture.
- The Myelencephalon.
- The Metencephalon.
- The Mesencephalon.
- The Diencephalon.
- The four transitional relays of the Siencephalon.
These systems do not merely receive biological information.
- They organise it.
- They structure it.
- They integrate it.
They convert biological conditions into behavioural trajectories.
Behavioural-Memory therefore represents the architectural organisation of perception, movement, orientation, timing, saliency, pattern detection, and behavioural continuity.
Unlike Biological-Memory, Behavioural-Memory exists behind the blood-brain barrier. It is embedded within neural organisation. Its properties cannot be extracted from blood chemistry. The behavioural architecture of an individual cannot be measured by examining liver enzymes or inflammatory proteins.
The diagnostic challenge becomes fundamentally different.
5. Behavioural Disorders as Spectral Variations
Conditions such as autism, schizophrenia, developmental syndromes, sensory integration disorders, neurodivergent, and other behavioural variations occupy the behavioural stratum.
These conditions are not failures of the liver. They are not failures of the kidneys. They are not failures of blood chemistry. They are variations within cephalic organisation. They emerge from inherited spectral differences across the subcortical gateways and their associated integration systems.
Because these systems operate through behavioural architecture rather than fluid chemistry, their diagnosis requires behavioural measurement.
- Temporal processing.
- Sensory integration.
- Spatial organisation.
- Attentional gating.
- Synchronisation dynamics.
- Structural connectivity.
- Behavioural trajectory mapping.
These diagnostic methods examine the organisation of Behavioural-Memory itself rather than the metabolic outputs of Biological-Memory.
The behavioural disease process therefore resides in an entirely different anatomical layer.
6. The Migration of Memory
A critical transformation occurs when biological information enters the cephalic systems. The information is no longer operating within peripheral tissue. It is now operating within specialised neural architecture. This migration changes the nature of the memory.
Behavioural-Memory retains the foundational properties of Biological-Memory. However, it acquires additional constraints unique to the central nervous system.
- Neural cell adhesion systems.
- Specialised glial interactions.
- Blood-brain barrier isolation.
- Unique immune regulation.
- Distinct developmental pathways.
- Gateway-specific organisational structures.
The result is a fundamentally different class of memory.
Behavioural-Memory emerges from Biological-Memory, but becomes something more than Biological-Memory. It becomes capable of integration.
- Prediction.
- Sequencing.
- Navigation.
- Attention.
- Behavioural display.
The reverse relationship does not occur. Biological-Memory cannot independently generate behavioural architecture. The migration is directional. Not reciprocal.
7. Emotional-Memory: The Isolated Weighting Engine
Above both Biological-Memory and Behavioural-Memory resides a third and entirely distinct layer.
Emotional-Memory.
This layer belongs to the Amygdala.
Within Psychextrics, the Amygdala functions as the Emotional Prioritisation Engine.
- Its purpose is not to create behaviour.
- Its purpose is not to reconstruct memory.
- Its purpose is not to generate consciousness.
Its function is weighting.
The Amygdala assigns:
- Threat value.
- Attraction value.
- Urgency.
- Familiarity.
- Novelty.
- Reward potential.
- Behavioural saliency.
Emotion therefore functions as a prioritisation mechanism. Not merely a feeling state.
The Amygdala determines which behavioural reconstructions receive access to expression.
- Which memories become vivid.
- Which memories remain dormant.
- Which perceptions become dominant.
- Which experiences command attention.
The emotional layer acts as a gatekeeper controlling access to behavioural display.
8. Why Emotional-Memory Is Isolated
A defining feature of Emotional-Memory is its relative autonomy from Behavioural-Memory.
The Amygdala does not merge its cellular architecture with the underlying behavioural pathways. But it emerge from the peripheral biological systems of Biological-Memory. It functions as an independent weighting engine for Behavioural-Memory.
Behavioural-Memory may contain thousands of possible reconstructions or potential behavioural possibilities within the organism. The Amygdala determines which become active.
A behavioural pathway without emotional weighting remains inactive. A behavioural pathway supplied with emotional valence becomes activated behavioural trajectory. The Behavioural-Memory itself may exist. Yet without emotional activation it will never reach conscious significance.
This explains why emotional events often become disproportionately memorable. The memory was not necessarily reconstructed differently. It was weighted differently. The Amygdala amplified its priority.
9. The Diagnostic Taxonomy of Memory
The tripartite model produces a corresponding tripartite diagnostic framework.
Biological-Memory is diagnosed through fluid analysis.
- Blood tests.
- Hormonal assays.
- Metabolic profiling.
- Inflammatory markers.
- Cellular outputs.
Behavioural-Memory is diagnosed through cephalic analysis.
- Sensory integration metrics.
- Behavioural profiling.
- Temporal processing measurements.
- Structural imaging.
- Connectivity mapping.
- Synchronisation studies.
Emotional-Memory requires an entirely different approach. Its activity must be inferred through amygdalar saliency mapping.
- Valence reactivity.
- Threat processing.
- Reward sensitivity.
- Behavioural prioritisation patterns.
- Neurotransmitter receptor distributions.
Each layer therefore demands its own diagnostic methodology because each layer operates according to its own biological laws.
10. Disease Across the Memory Hierarchy
Disease can emerge at any point within this hierarchy.
- Biological diseases emerge from failures within peripheral memory systems.
- Behavioural disorders emerge from alterations within cephalic memory systems.
- Emotional disorders emerge from distortions within the amygdalar weighting engine.
Although these layers interact continuously, pathology often reveals where the disruption originates.
- A metabolic disease may profoundly alter behaviour.
- A behavioural disorder may alter emotional weighting.
- An emotional disturbance may reshape biological physiology.
Yet each disturbance can still be traced back to its dominant memory stratum.
The tripartite model therefore provides a unified framework through which both health and disease can be interpreted with precision.
Conclusion: The Biological Staircase of Memory
The tripartite stratification of memory reveals that behaviour emerges from a layered biological hierarchy rather than a singular psychological construct.
Biological-Memory forms the foundation. It records the living history of the organism through cellular and molecular architecture.
Behavioural-Memory forms the middle layer. It transforms biological history into organised patterns of perception, orientation, integration, and action.
Emotional-Memory forms the regulatory summit. It assigns priority, urgency, significance, and saliency to behavioural possibilities.
Together these three systems create the complete architecture of memory within Psychextrics.
- The blood diagnoses the body.
- The cephalic gateways diagnose behaviour.
- The Amygdala governs emotional expression.
- The Hippocampus reconstructs behavioural continuity.
- The Thalamus narrates symbolic meaning.
- And the Telencephalon displays the final conscious reality.
Memory is therefore not a single phenomenon. It is a biological staircase through which life becomes behaviour, behaviour becomes meaning, and meaning becomes conscious experience.
Back to: 👇