Henry Molaison Revisited: The Case That Defined Memory Research—and Why It May Need Reconsideration
BY: OMOLAJA MAKINEE
Few individuals have influenced modern Neuroscience as profoundly as Henry Gustav Molaison. For decades, he was known simply as “H.M.”, a patient whose unusual neurological condition transformed scientific understanding of memory and helped establish the modern distinction between different memory systems.
His case appears in countless textbooks, university lectures, documentaries, and neuroscience blogs. Yet despite its fame, much of the public understanding of Henry Molaison remains frozen in an earlier version of the story.
Following his death and the subsequent re-examination of his brain, several important anatomical findings emerged that complicated the traditional narrative. These findings do not diminish the significance of the case. Rather, they reveal that many simplified conclusions drawn from H.M. deserve closer scrutiny.
The purpose here is not to reject the importance of Henry Molaison. It is to revisit the historical record in full, distinguish established facts from later interpretations, and explore why the case remains relevant to alternative frameworks such as Psychextrics.
1. The Man Behind the Initials
Henry Gustav Molaison was born on February 26, 1926, in Manchester, Connecticut. By all available accounts, he experienced a relatively ordinary childhood. He attended school, interacted normally with family and friends, and exhibited no signs of severe cognitive impairment.
During childhood, however, he reportedly suffered a bicycle accident involving a blow to the head. Whether this incident contributed directly to his later neurological condition remains uncertain, but it has often been discussed within historical accounts of his life.
As he entered adolescence, Henry began experiencing epileptic seizures. Initially mild, the seizures gradually increased in both frequency and severity. By adulthood they had become debilitating.
The condition interfered with:
- Employment.
- Social activities.
- Daily functioning.
- Long-term independence.
By the early 1950s, available treatments had failed to control his epilepsy effectively. Faced with increasingly severe seizures, Henry and his family agreed to pursue an experimental surgical intervention.
2. The Surgical Decision
At the time, neurosurgical knowledge was still developing. Brain imaging technologies that are commonplace today did not yet exist.
Henry came under the care of neurosurgeon William Beecher Scoville, who believed that removing portions of the medial temporal lobes might reduce seizure activity.
The operation was experimental. The exact consequences were unknown. The primary goal was simple:
To reduce or eliminate the epileptic seizures that had come to dominate Henry’s life.
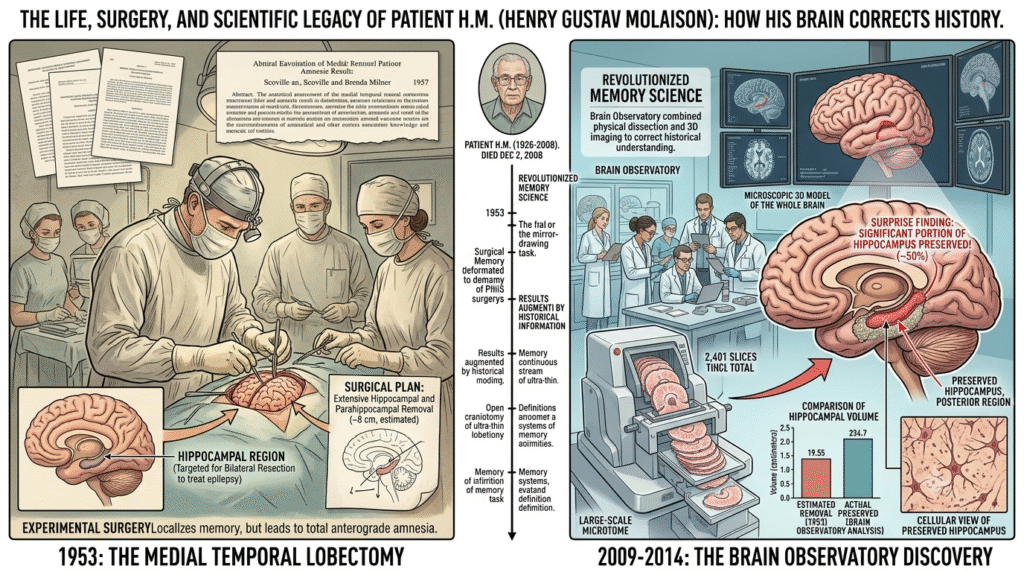
In 1953, at twenty-seven years old, Henry underwent surgery.
3. The Operation of 1953
The operation involved the bilateral removal of substantial portions of the medial temporal lobes. For many years, textbooks described the procedure as the removal of the hippocampus. This description became one of the most repeated statements in neuroscience.
However, subsequent investigations revealed that the surgery affected much more than the hippocampus alone.
The procedure removed or damaged portions of:
- The hippocampus.
- The entorhinal.
- The parahippocampal region.
- The amygdala.
- Adjacent medial temporal structures.
- Associated white matter pathways.
The surgery achieved its primary objective. Henry’s epilepsy improved dramatically. Yet an entirely unexpected outcome emerged.
4. The Discovery
After surgery, Henry appeared remarkably normal in many respects. He could:
- Speak fluently.
- Understand language.
- Engage in conversation.
- Perform routine activities.
- Recall many events from his childhood and early adulthood.
Yet something fundamental had changed. He could no longer reliably form new long-term autobiographical memories.
- Visitors could introduce themselves. Minutes later, he might not remember meeting them.
- Researchers could spend hours conducting experiments with him. The following day he often had no recollection of ever participating.
This condition became known as profound Anterograde Amnesia.
The discovery transformed Neuroscience. It suggested that memory was not a single unified function but a collection of specialised processes.
5. Life After the Operation
One of the most remarkable aspects of Henry’s life after surgery was how much remained intact.
His intelligence remained largely preserved. His language abilities remained functional. His personality remained stable. Observers frequently described him as polite, cooperative, friendly, and patient. Perhaps most surprising was the discovery that Henry could still learn.
Researchers taught him various motor tasks. One of the most famous involved mirror drawing. With repeated practice, his performance improved significantly. Yet he consistently denied ever having performed the task before.
His body appeared capable of improvement. His autobiographical awareness of that improvement did not develop in the same way.
For decades this observation became a cornerstone of memory research.
6. The Longest Experiment in Neuroscience
Over the following fifty-five years, Henry became one of the most studied individuals in scientific history. Researchers repeatedly examined:
- Memory.
- Learning.
- Language.
- Perception.
- Motor behaviour.
- Social interaction.
His case profoundly influenced modern theories of:
- Episodic memory.
- Procedural memory.
- Declarative memory.
- Memory consolidation.
For much of this period, the scientific community knew him only by his initials: H.M. His identity remained confidential until after his death.
7. What Happened After His Death?
Henry Molaison died on December 2, 2008.
Following his death, neuroscientists undertook one of the most detailed anatomical investigations ever performed on a human brain. The brain was scanned, sectioned, digitised, and reconstructed in extraordinary detail. What emerged was significant.
The post-mortem analysis revealed that the traditional textbook description was incomplete. The operation had not created a clean lesion. Instead, it produced a far more complex anatomical outcome.
Researchers discovered:
- The hippocampus had not been completely removed.
- Portions of posterior hippocampal tissue remained.
- Portions of the amygdala remained.
- Portions of the entorhinal system remained.
- Numerous surrounding medial temporal structures were partially preserved.
- Multiple connecting pathways had been altered.
- The surgery represented a mixed lesion rather than a selective hippocampal excision.
These findings fundamentally complicated decades of simplified explanations.
8. Why This Matters
Many Neuroscience articles continue to present H.M. as proof that memory exists outside the hippocampus because “his hippocampus was removed yet old memories survived.”
The problem is that the anatomical record no longer supports such a simplified statement. The post-mortem evidence demonstrates that:
- Hippocampal tissue remained.
- Entorhinal tissue remained.
- Amygdalar tissue remained.
- Medial temporal circuitry remained partially operational.
Consequently, the case cannot conclusively establish that memory was relocated elsewhere. Nor can it conclusively establish that the hippocampus functions as a memory storage vault.
What the case actually demonstrates is more limited but perhaps more important:
Severe disruption of the medial temporal anchoring architecture profoundly impairs the formation of new autobiographical experiences.
Beyond that conclusion, interpretation becomes increasingly theoretical.
9. The Psychextric Criticism
Within Psychextrics, the H.M. case is viewed differently.
The criticism is not directed at Henry Molaison himself nor at the quality of the original observations. The criticism is directed at how later generations interpreted those observations.
The traditional narrative often assumes:
- The hippocampus was removed.
- Old memories survived.
- Therefore memory must be stored elsewhere.
Psychextrics argues that this reasoning moves beyond what the evidence actually proves. The post-mortem findings reveal that critical structures remained partially intact.
As a result, H.M. does not provide evidence that memory survived without hippocampal participation. Instead, the case may demonstrate the consequences of damaging a primary anchoring architecture while leaving portions of that architecture operational.
From a Psychextric perspective:
The hippocampus is not a repository of memory.
It is the primary anchoring architecture through which distributed biological modifications become reconstructable as autobiographical experience.
This distinction is important.
A storage model asks: “Where is memory kept?“
An anchoring model asks: “How is experience reconstructed?“
The H.M. case may ultimately tell us less about storage and more about reconstruction.
Conclusion: The Question That Remains
More than seventy years after the surgery, Henry Molaison continues to shape discussions of memory. Yet the most important lesson of his case may not be the answer it provided. It may be the question it left unresolved.
If memories are not stored as complete recordings within a single structure, how does the brain reconstruct a coherent sense of personal history?
The updated anatomical record shows that the answer cannot be reduced to a single organ.
- The hippocampus mattered.
- The entorhinal mattered.
- The amygdala mattered.
- The surrounding medial temporal system mattered.
- The pathways connecting them mattered.
Henry Molaison remains one of the most important figures in Neuroscience not because he solved the mystery of memory, but because his life revealed how much of that mystery still remains.
Back to: 👇